Specialty Contact Lenses
In early-stage keratoconus, glasses or astigmatic soft contact lenses can correct vision. As the condition progresses, hard (RGP) lenses, hybrid lenses, or scleral lenses are used for correction.

Backed by proven expertise, we safeguard your eye health with confidence
Keratoconus is a progressive disorder in which the cornea abnormally thins, loses its smooth round shape, and bulges forward — producing irregular astigmatism. Its prevalence is roughly 0.15% to 0.6% of the general population. It typically begins in the teens, with an average age of onset of 16. It is bilateral in most cases (90%) but starts asymmetrically; the second eye usually develops the condition about 5 years later.
The condition typically progresses actively for 5 to 7 years and then stabilizes. In recent years, post-LASIK/LASEK ectasia — also called keratoectasia — has been reported as a side effect of refractive surgery.
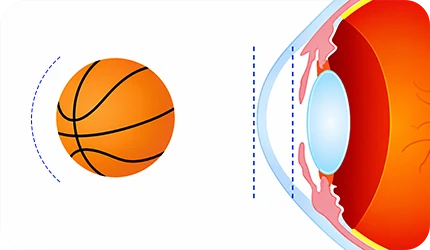
Normal
Keratoconus
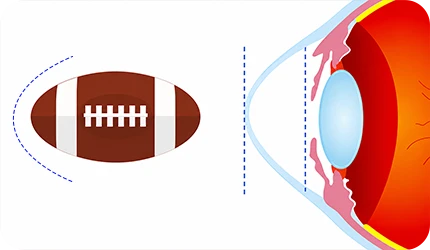
Normal
Keratoconus
The exact cause of keratoconus is not yet established and remains hypothetical. The most strongly supported hypotheses include congenital genetic predisposition (heritability is not clearly established but is estimated at around 6–8%), associated systemic conditions (atopic disease, allergic rhinitis, Down syndrome), and habitual eye rubbing.

Patients with keratoconus typically experience blurred vision, diplopia, myopia, and irregular astigmatism (usually bilateral, though severity may differ between eyes). Glasses provide poor correction, and amblyopia may develop. In severe cases, corneal hydrops can cause pain, tearing, and scarring, leading to secondary infection.
Diagnosis is made through slit-lamp biomicroscopy, retinoscopy, keratometry, specular biomicroscopy, and corneal topography. Topography (TOPO) is particularly useful for detecting early keratoconus by identifying suspicious patients through quantitative measurements. However, conventional TOPO only images the anterior cornea, which can make ambiguous or early-stage cases difficult to diagnose.
JC Bitsomang Eye Clinic uses the Galilei G4, which images both the anterior and posterior cornea — enabling more accurate evaluation of subclinical keratoconus.

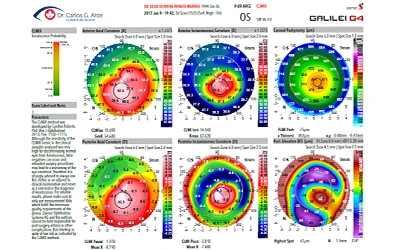
Galilei G4

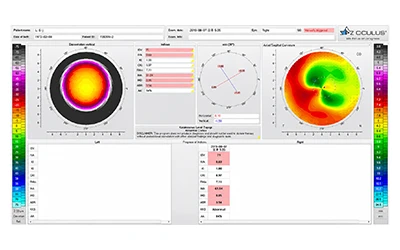
K5M
Keratoconus has four progressive treatment stages: glasses, then specialty lenses, Intacs ring segments, collagen cross-linking, and finally corneal transplantation.
In early-stage keratoconus, glasses or astigmatic soft contact lenses can correct vision. As the condition progresses, hard (RGP) lenses, hybrid lenses, or scleral lenses are used for correction.


Keraring or Intacs ring segment implantation in the corneal stroma is a procedure for keratoconus patients whose vision cannot be corrected by contact lenses or who cannot tolerate them — typically performed before considering corneal transplantation. · Slows progression of keratoconus and helps prevent transplantation · No damage to corneal tissue · Short surgical and recovery time · Proven safety profile · Long-term clinical outcomes and effectiveness
The cornea is composed of collagen tissue and corneal stromal cells, layered in an interlocking structure that maintains its shape. In keratoconus patients, the cohesion of collagen is weaker than normal, causing the cornea to deform into a cone shape. Cross-Linking strengthens the corneal structure by saturating the cornea with riboflavin (Vitamin B2) and exposing it to UV-A light. The riboflavin, activated by UV light, increases corneal collagen bonding strength by approximately 300%. Care must be taken when corneal thickness is below 400μm, as this can risk damage to intraocular tissues. Cross-Linking provides an average reduction of about 1.5D (up to 3–4D) in corneal refractive power.




When keratoconus has progressed severely, penetrating or lamellar corneal transplantation is performed. Transplantation is the final treatment stage. Penetrating Keratoplasty (PKP) involves removing and replacing the full thickness of an approximately 8mm donor cornea. Deep Anterior Lamellar Keratoplasty (DALK), a partial transplant, replaces the corneal layers from above Descemet's membrane through the epithelium. Because DALK preserves the patient's own Descemet's membrane and endothelium, it has lower rejection rates than PKP, sutures can be removed earlier (reducing induced astigmatism), and the risks of suprachoroidal hemorrhage (SCH), infection, and steroid side effects are lower.








