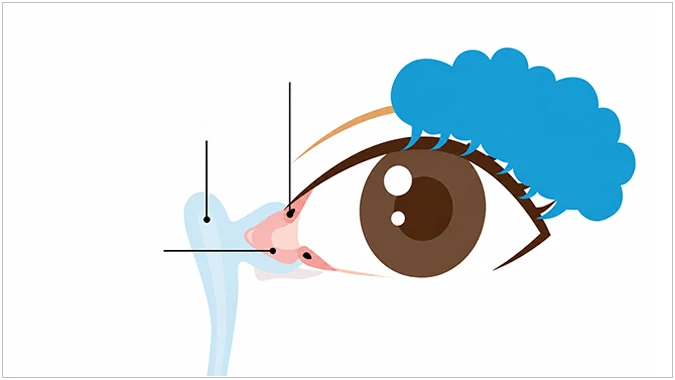





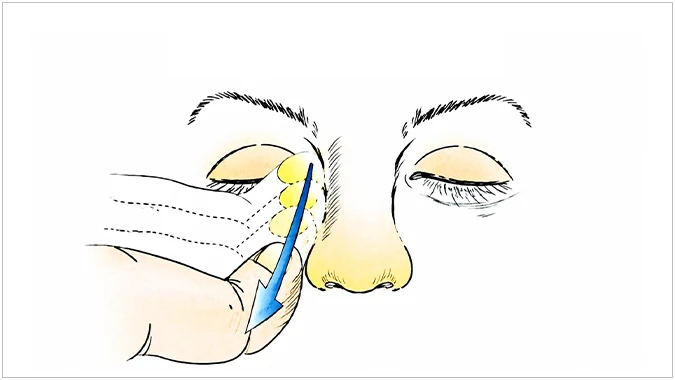
Example of massage method
Lacrimal sac massage with antibiotic drops
For congenital epiphora the first-line treatment is non-surgical massage. It is mainly performed in infants under 5 months: pressing on the canaliculi with the index finger prevents reflux from the puncta while increasing pressure inside the sac and duct, which can rupture the membranous obstruction at the nasal end. When purulent discharge is severe, antibiotic drops or ointment are added. Approximately 90% of cases improve within the first 6–12 months of life.