
Vision Correction Center
Trusted expertise to safely care for your eye health.
Rigid Gas-Permeable (RGP) Lens
A gas-permeable lens with the lowest risk of adverse effects
Rigid gas-permeable (RGP) contact lenses transmit oxygen directly through the lens material, providing ample corneal oxygenation and minimizing adverse effects. Unlike soft contact lenses, RGP lenses do not adhere to the corneal surface but float on the tear film during refractive correction, and are particularly effective for astigmatism correction. The lens is custom-fitted to each patient's corneal topography and dimensions. Among non-surgical refractive correction options other than spectacles, the RGP lens offers the most favorable ocular-health profile.


Soft Lens vs RGP Hard Lens
| Parameter | Soft Lens | RGP Hard Lens |
|---|---|---|
| Peripheral visual field | Wide | Narrow |
| Corneal oxygen permeability (Dk/t) | Low | Very high |
| Dryness sensation | Varies by polymer material | Minimal |
| Tear-film exchange | Limited | Excellent |
| Wearing comfort | Excellent | Initial discomfort |
| Maintenance requirement | Less critical (scheduled replacement) | Requires consistent daily care |
| Adaptation period | Quick | 1–2 weeks minimum |
| On-eye positional stability | Stable | May dislodge with vigorous movement |
| Astigmatism correction | Less complete | Superior |
| Patient suitability | Most patients without severe dry-eye syndrome | Requires careful corneal topographic assessment |
RGP Lens Adaptation Protocol



A corneal adaptation period is required.
First-time RGP lens wearers typically experience mild foreign-body sensation and increased ocular strain for several days, so extended wear from day one is not advisable. A gradual lens-wear schedule allowing the cornea to adapt is therefore required. While individual response varies, foreign-body sensation generally subsides within 4–5 days. After 1–2 weeks, the majority of patients can comfortably wear the lens throughout the day.
Soft Contact Lens
The most accessible form of refractive correction
Soft contact lenses, fabricated from flexible hydrogel or silicone-hydrogel polymers, are the most widely prescribed contact lenses due to their ease of insertion and care. With high water content and a pliable lens material, soft lenses offer superior wearing comfort relative to other lens modalities. However, even the most advanced soft lens delivers less corneal oxygenation than an RGP lens, so it is generally unsuitable for patients with dry-eye syndrome or those routinely in low-humidity environments.


Essential clinical considerations before selecting a Soft Lens
Water Content
Soft contact lenses inherently contain a substantial proportion of moisture within the polymer matrix; this ratio is termed the water content. Patients with dry eyes should be fitted with low-water-content lenses, while those with abundant tear secretion are better served by high-water-content lenses. At JC Bitsomang, precision tear-film analysis with our Tear Film Analyzer enables accurate selection of the appropriate water content tailored to each individual.
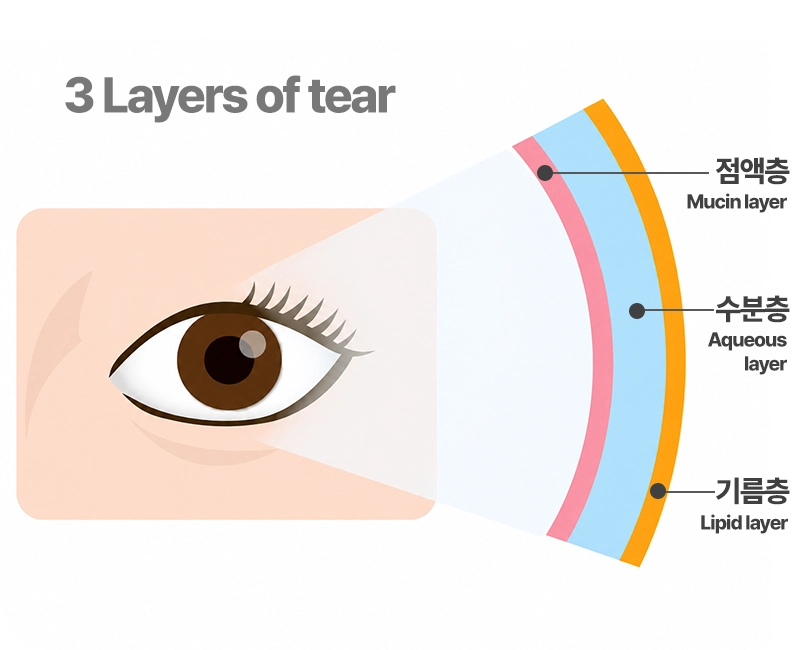
- Mucin Layer
The innermost layer of the tear film. It distributes the tears evenly across the corneal surface where the lens contacts the eye, and smooths the irregular corneal epithelial surface to enable clear vision.
- Aqueous Layer
The thickest middle layer of the tear film. Dissolved oxygen and nutrients diffuse from this layer to the cornea, maintaining ocular surface cleanliness and flushing impurities from the conjunctival sac.
- Lipid Layer
The outermost layer of the tear film. It prevents tear evaporation into the air and serves as a lubricant between the eyelid and cornea during blinking, reducing ocular discomfort.
Lens Diameter & Base Curve
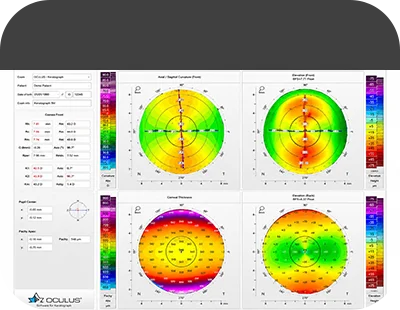
Because the eyeball is approximately spherical, the contact lens is correspondingly curved to conform. Just as no two individuals share identical facial features, fingerprints, or stature, each eye displays subtle variations in corneal shape, size, and curvature, so a pre-fitting examination is essential to prescribe the lens diameter and base curve specifically tailored to each patient.
Soft Contact Lens Modalities
Daily Disposable (toric available)
Bi-weekly (toric available)
Monthly (toric available)
Quarterly / Annual (toric available)
Cosmetic Color Lens
Prosthetic Iris Lens
Toric Soft Lens (Astigmatism)
Because the eye is not a perfect sphere but rather an oblate ellipsoid, incoming light is dispersed and images appear blurred — this refractive error is termed astigmatism. The toric soft lens is specifically prescribed for patients whose astigmatism is significant enough that correcting only myopia or hyperopia would leave residual visual blur.

Silicone Hydrogel Lens
A next-generation soft lens engineered with novel silicone-hydrogel polymers to overcome the limitations of conventional soft lenses (PMMA material). It addresses the long-standing issues of oxygen permeability and dryness, enabling extended wear with reduced ocular irritation and minimal conjunctival hyperemia even after prolonged use.

Prosthetic Iris (IRIS) Lens
A specialized soft lens used for cosmetic and prosthetic indications by patients who have lost vision or whose iris coloration or shape is abnormal due to trauma or disease. The lens incorporates a prosthetic iris pattern that fully conceals the underlying defect, with color shading customizable in graded steps according to each patient's ocular condition.
Long-term Storage Protocol
When storing contact lenses, thoroughly clean and rinse the lenses, then place them separately in a marked L/R lens case using dedicated multi-purpose preservative solution. When lenses are immersed in preservative solution, the solution must be replaced every 2–3 days. Failure to replace the solution may lead to lens contamination, so when lenses will not be used for an extended period, follow the storage protocol below.
- After cleaning, air-dry the lenses for 5–6 hours away from direct sunlight.
- Store in a fresh case without solution.
Recommended For
First-time contact-lens wearers; patients with irregular corneal topography; occasional wearers; athletes engaged in vigorous physical activity; individuals in dusty environments or industrial settings; patients with large or decentered pupils; and those with incomplete lid closure (lagophthalmos) or proptotic eyes








