Retina & Glaucoma Center
Trusted expertise to safely protect your eye health.
Glaucoma Treatment
Intraocular pressure (IOP) is managed mainly through three modalities — medication, laser, and surgery. Once diagnosed, glaucoma requires lifelong continuous care. Proper IOP control prevents further optic nerve damage and protects against visual field and acuity loss.
Laser Treatment
Laser modifies intraocular structures to lower IOP. It is indicated for angle-closure glaucoma and for open-angle glaucoma that does not respond to medication. Mild discomfort, foreign-body sensation, or a transient IOP rise may occur, and medication or surgery may be added if IOP is not adequately controlled. Most procedures are performed in a dedicated laser room rather than the operating room; some refractory cases are treated in the OR.
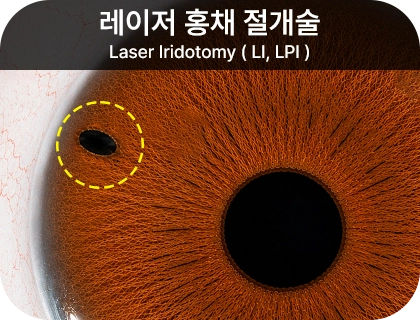
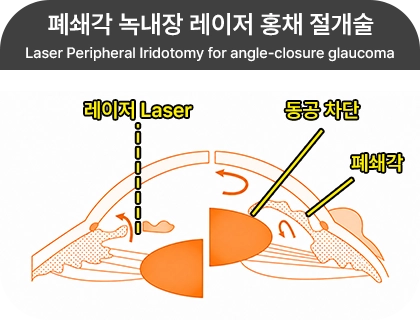
Laser Iridotomy (LI / LPI)
When angle-closure glaucoma blocks the circulation of aqueous humor, laser is applied at the peripheral iris to create a drainage channel that lowers IOP. It is commonly used for acute or chronic angle-closure glaucoma. The procedure is performed in the outpatient clinic under topical anesthesia. Transient IOP elevation, corneal pain from the laser, and — rarely — anterior chamber bleeding or anterior uveitis with mild vision reduction may occur, but these typically resolve within a few days. Iridotomy also reduces the risk of acute angle-closure attacks triggered by moderate pupil dilation in dim light or during near work.
Laser Trabeculoplasty
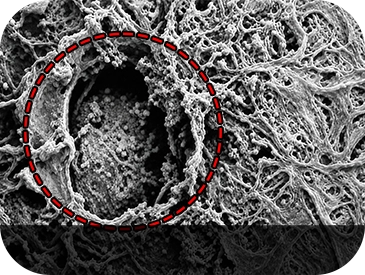
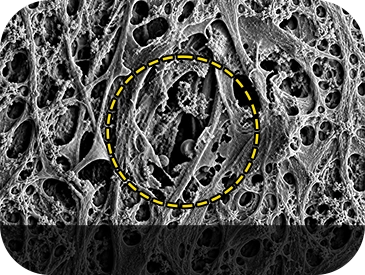
Laser is applied to the trabecular meshwork — the aqueous outflow pathway — to increase outflow and lower IOP. It is most often used in primary open-angle glaucoma when maximum medical therapy fails to adequately control pressure. The procedure is performed in the outpatient clinic under topical anesthesia.
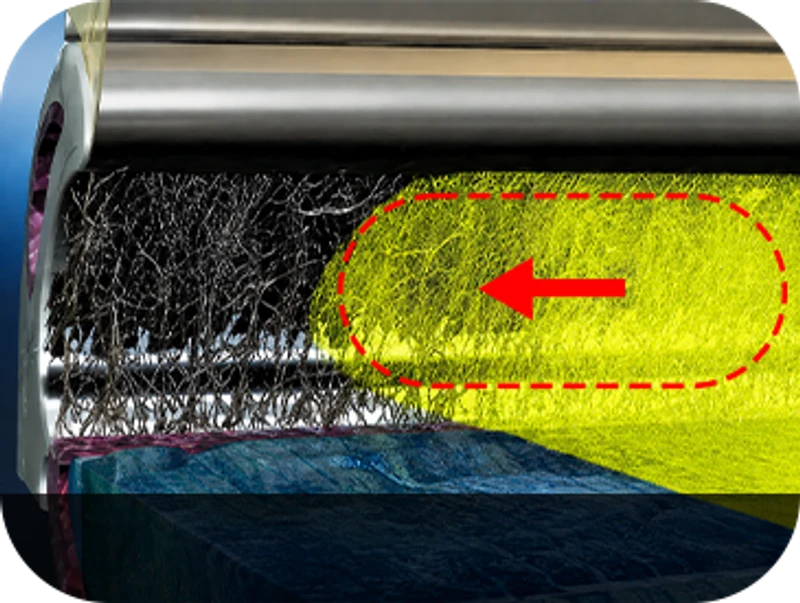
SLT (Selective Laser Trabeculoplasty)
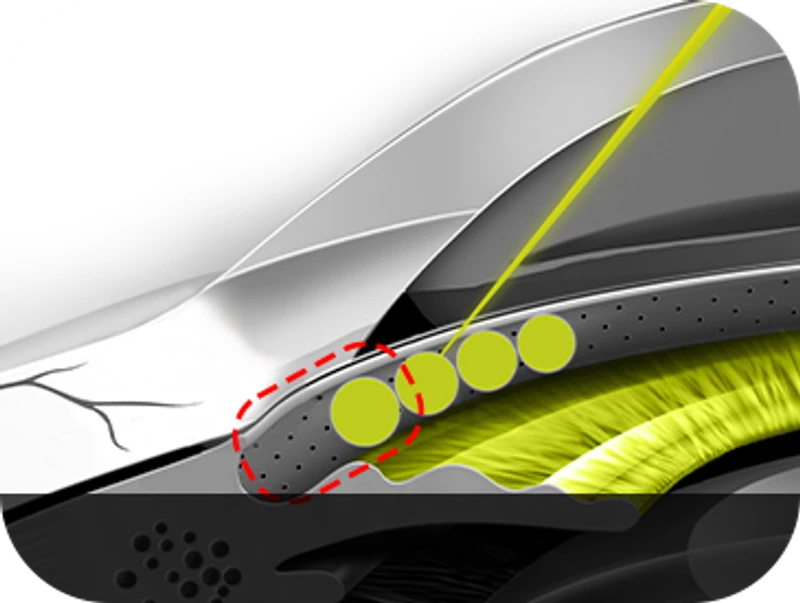
SLT selectively targets pigmented (melanin-containing) cells within the trabecular meshwork. By delivering a specific wavelength of laser for an extremely brief duration, only the dysfunctional pigmented cells are removed — without damaging surrounding tissue — lowering IOP. This is a novel selective approach to glaucoma laser therapy that resolves the impaired outflow at its source. Brief laser pulses widen the outflow channels and produce IOP reduction in approximately 70–80% of cases. Because the energy is low and selectively absorbed by pigmented cells, the surrounding tissue is essentially spared, allowing the procedure to be safely repeated.

SLT procedure
»
The procedure takes about 2 minutes for both eyes and is painless. You can return to daily activities right after.
Starting the next day, regular follow-ups over several weeks monitor changes in eye condition and IOP.
Topical Anesthesia
SLT Laser Application
1 min / eye!
Anti-inflammatory Eye Drops
Pros of SLT Laser
»- No systemic side effects.
- Procedure takes under 1 minute per eye, with virtually no pain. (per eye)
- A single session sustains IOP-lowering for several years. (individual variation applies)
- Extremely safe — pulse duration is only 4 ns* (0.000000004 sec).
- No collateral trabecular damage, so the laser can be repeated
- Covered by Korean national health insurance.
Prosof SLT Laser
»
- No systemic side effects.
- Procedure takes under 1 minute per eye, with virtually no pain. (per eye)
- A single session sustains IOP-lowering for several years. (individual variation applies)
- Extremely safe — pulse duration is only 4 ns* (0.000000004 sec).
- No collateral trabecular damage, so the laser can be repeated
- Covered by Korean national health insurance.
Surgical Treatment
Surgery is performed when medication is ineffective, when medication alone cannot lower IOP sufficiently, when the patient's response to medication is poor, or when medical therapy is otherwise difficult. For certain glaucoma types it is also used as a first-line option. These procedures create a drainage pathway so that aqueous humor exits along the outer wall of the eye in a controlled manner — examples include trabeculectomy and aqueous shunt implantation. Postoperative care has a critical impact on IOP control. Complications such as IOP elevation, hypotony, intraocular hemorrhage, or endophthalmitis may occur, so continued monitoring and treatment are required. Depending on the case, laser suture lysis or ocular digital massage may be needed under your surgeon's direction. For one month after surgery, avoid touching or rubbing the eye with unclean hands and any activity that could cause infection or trauma to the surgical site.

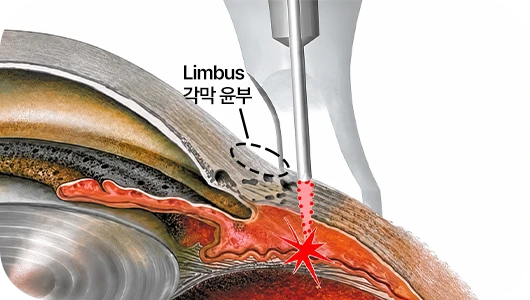
XEN Gel Stent
The XEN gel stent is a surgical implant designed to lower elevated IOP in open-angle glaucoma patients in whom prior treatment has failed or medication alone is insufficient. It has cleared US FDA clinical trials, with established safety and efficacy. Designed to remain permanently in the eye, the XEN stent is a small ~6 mm tube made of biocompatible material that becomes soft and pliable after implantation. The procedure is performed under topical anesthesia using a fine-needle inserter that places the stent into the subconjunctival space. The XEN stent implantation requires only a ~2.2 mm incision — just large enough for the inserter needle — and no sutures are needed. IOP lowering is comparable to trabeculectomy, with faster recovery and fewer side effects.
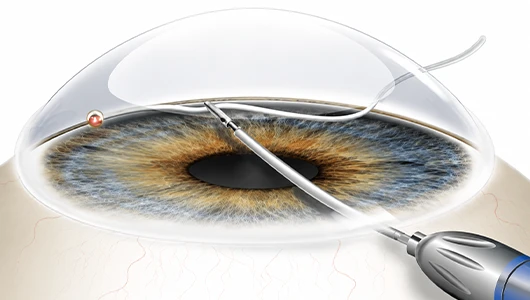
Trabeculectomy
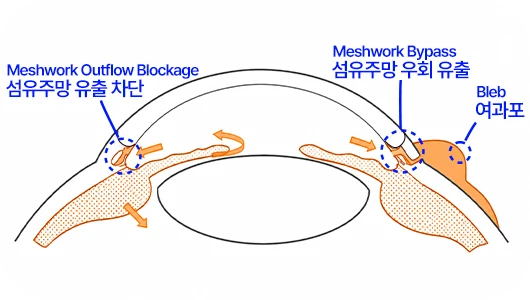
Trabeculectomy has long been one of the most widely used surgical methods for glaucoma. It creates a drainage channel and a filtering bleb beneath the conjunctiva so that aqueous humor can exit at a controlled rate, lowering IOP. The procedure does not eliminate glaucoma itself but is performed to control IOP when other approaches are insufficient.
Cyclophotocoagulation (CPC)
Laser energy is delivered to the ciliary processes — the structures that produce aqueous humor — destroying them to suppress aqueous production. Because it can damage the eye itself and trigger inflammatory complications, it is generally reserved as an adjunctive IOP-control method in patients who have failed multiple prior surgeries or for whom incisional surgery is contraindicated.
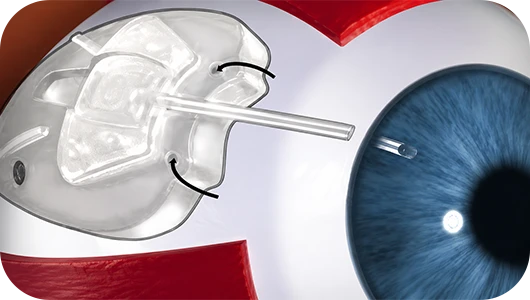
Aqueous Shunt — Ahmed Valve Implantation
Aqueous shunt implantation has become one of the more frequently used options for glaucoma with high IOP. It yields relatively favorable outcomes in cases where conventional trabeculectomy fails to control pressure with medication and the prognosis is otherwise unfavorable — including secondary glaucoma and reoperation cases. The shunt device is placed beneath the conjunctiva to create a controlled outflow pathway for aqueous humor, lowering IOP. The procedure does not eliminate glaucoma itself but is performed to control IOP when other methods are insufficient.
Combined Cataract–Glaucoma Surgery (Phacotrabeculectomy)
Cataract clouds the crystalline lens and reduces visual acuity; glaucoma narrows the visual field through elevated IOP and other mechanisms. Glaucoma patients commonly develop secondary cataract from prolonged IOP-lowering medication or prior glaucoma surgery. When both conditions coexist, trabeculectomy can be performed during cataract surgery in a single combined procedure. Cataract surgery removes the clouded lens and implants an intraocular lens through a small scleral incision. The same site is used to create a controlled aqueous drainage bleb for IOP management; a separate drainage channel may also be created in selected cases. This combined surgery aims to control IOP efficiently after cataract removal. Compared with routine cataract surgery, postoperative monitoring and care are particularly important — IOP stabilizes only after a certain period and visual recovery is slower than with conventional cataract surgery.








