
Cataract & Presbyopia Center
Trusted expertise to safely care for your eye health.
Complex Cataract Surgery

On-site retina diagnostics and surgical facilities at JC Bitsomang Eye Clinic
Although rare, dense or long-standing cataracts increase the risk of intraoperative posterior capsular rupture and IOL dislocation. Prompt management of these complications leads to better visual outcomes, and retinal involvement in particular often constitutes a surgical emergency that demands immediate intervention.
These postoperative complications are uncommon, but depending on the condition and severity, timely and appropriate treatment is essential. Most cases recover fully, although in rare instances such as severe retinal detachment or refractory endophthalmitis, full visual recovery may not be achievable.
Most clinics refer such cases to a university hospital.
JC Bitsomang Eye Clinic has an in-house retinal surgeon as well as full retinal diagnostic and surgical facilities, allowing intraoperative complications to be managed and operated on without complex referral procedures.
We also treat complications that arose from surgery performed at other clinics, doing our utmost to protect each patient's vision.
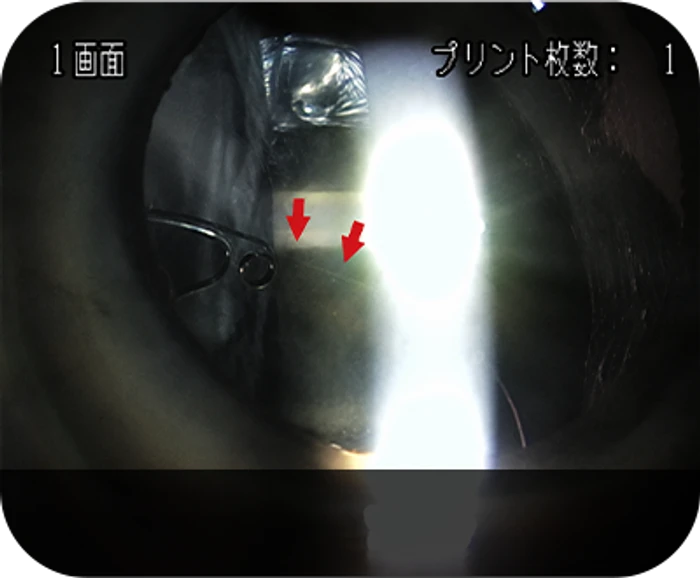
Posterior Capsular Rupture
During cataract surgery, the anterior capsule and natural lens are removed and replaced with an intraocular lens (IOL). Depending on the patient's ocular condition, the posterior capsule may rupture during this step. The reported incidence is around 1 – 2%, and once rupture occurs, prompt surgical management under the judgement of an experienced vitreoretinal surgeon is required to preserve vision and prevent further complications.
- Symptoms
· Sudden pupil dilation or change in pupil shape · Abrupt deepening of the anterior chamber during phacoemulsification · Unexplained, insufficient aspiration of lens fragments · Tilting of the lens equator · Sudden clearing of the posterior capsule or abrupt appearance of capsular wrinkles
- Treatment
When the posterior capsule ruptures, vitreous from behind the capsular bag prolapses into the anterior chamber, so an anterior vitrectomy is performed to remove the herniated vitreous.
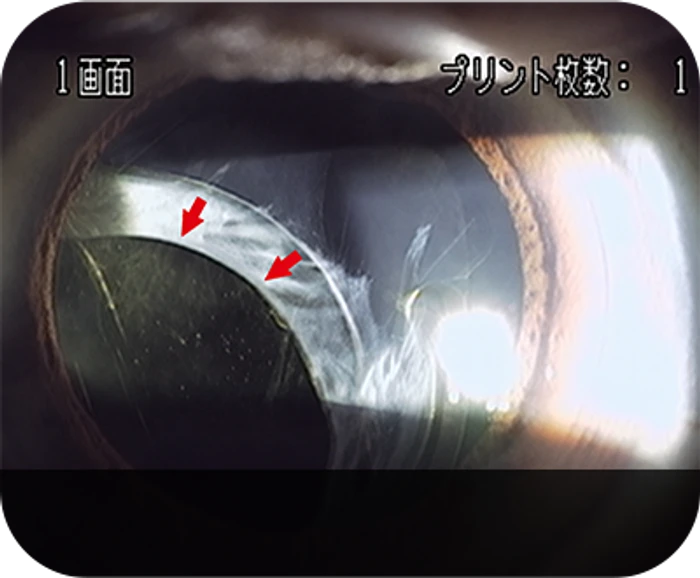
IOL Dislocation
IOL dislocation refers to displacement of the implanted intraocular lens from its intended position after cataract surgery. The reported incidence ranges from approximately 2 – 2.8%, and most cases present in the early postoperative period. Although an IOL is small, it has its own weight, so impact, vigorous physical activity, or zonular weakness (for example pseudoexfoliation or traumatic zonulopathy) can cause it to slip out of the capsular bag, decenter anteriorly toward the pupil, or sink into the vitreous cavity.
- Symptoms
Patients may experience blurred vision in proportion to the degree of dislocation; a partially decentered IOL may produce no noticeable symptoms. When the zonular fibers supporting the IOL are damaged, the iris also loses its support and may exhibit iridodonesis (a tremulous iris).
- Treatment
When the IOL is dislocated posteriorly and inaccessible from the anterior approach, a pars plana vitrectomy is performed followed by scleral fixation. When anterior access is feasible, IOL refixation techniques include scleral fixation, iris fixation, iris-sulcus fixation, or simple repositioning of the IOL without suture fixation; capsular tension rings (CTR), iris hooks and other adjuncts are used as indicated.
Sedation Anesthesia
Sedation anesthesia uses intravenous sedatives to relieve anxiety, tension, and pain during surgery, reducing patient discomfort and eye movement to create a more stable surgical environment. Unlike general anesthesia, it maintains spontaneous breathing while the patient's level of consciousness, vital signs, and oxygen saturation are monitored to adjust the depth of sedation. Beforehand, suitability is assessed by reviewing hypertension, diabetes, cardiovascular and respiratory disease, current medications, and anesthesia history; afterward, drowsiness, dizziness, and slowed reactions may persist, so driving on the same day should be avoided and being accompanied by a guardian is recommended.

- Sedation Anesthesia
Considered when surgery may take longer—such as retinal surgery—or when stable sedation management is needed given the patient's condition. It may also be performed when severe anxiety or tension causes eye movement or reduced cooperation.
- Local · Topical Anesthesia
Relatively short procedures such as cataract surgery can be performed with topical or local anesthesia alone. When the patient can cooperate and is in stable general condition, only the necessary area is anesthetized for the procedure.








